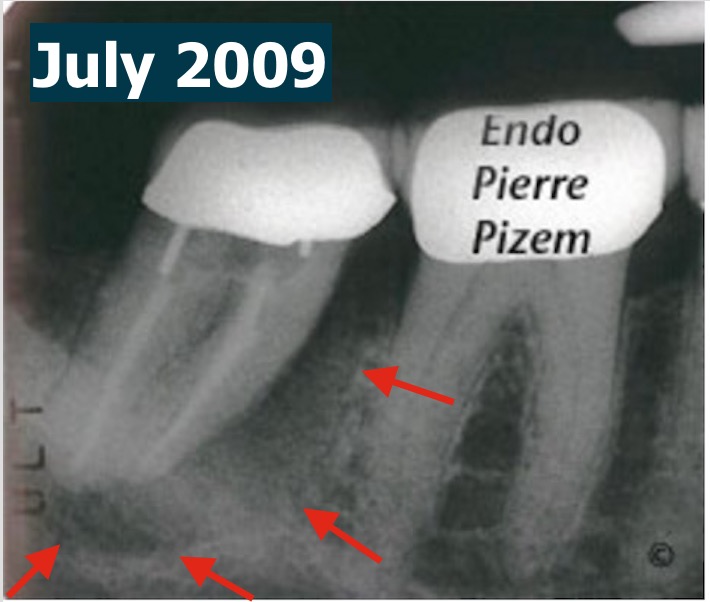
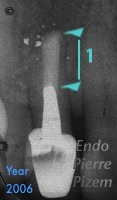
On July the 29th 2009, we have been presented with this mandibular second molar. Patient was experiencing pain. This radiographic image showed a
Thinking Out of the Box 20 years Ago to Preserve a Tooth! An Early Ceramic Material Apical Filling
Wide apical foramen, thin canal walls, necrotic pulp would, in year 2000, condemn this tooth and have it replaced by an implant supported
A Root Canal Retreatment Involving a Crown and a Post Removal Alowed for This Painful Tooth to be Preserved
An endodontist case report. MicroEndodontic. Case Study Number 505026 Twenty five years old patient presenting with an abscessed maxillary molar.
Pushing Back the Limit to Save Teeth with Opmi Proergo Dental Operative Microscope. Dental Operating Microscope Assisted Root Canal Procedure on a Completely Stenosed Canal System.
MicroEndodontic. Case Study Number 449947 Pulp chamber and root canals are not visible on pre operating X Ray of second mandibular molar. Diffuse
Endodontic Revision Procedure on Mandibular Molar, a 6 months Post Operative Outcome
Case Study Number 495336 Symptoms: Acute pain to pressure, patient is eating on the opposite side. Root canal was done three years ago. Tooth
Endodontic Treatment on Mandibular Molar with Calcified Canals and a “J” Type Lesion, a Five Years Follow Up
Root Canal Procedure with Surgical Operative Microscope. MicroEndodontic. Case Study Number 156037. Pre operative film shows a large bony
Sven-Erick Hamp Class III Furcation Defect? Parodontal Prognosis? A Seven years Follow Up
Preoperative X ray dental film shows a "furcation defect" encompassing the entire width of the tooth (no probing). A root canal treatment implying a
To Save or Not To Save? That Was the Question. A Seven Years Post Endodontic Treatment Outcome Follow Up
Case Study Number 368745 Patient was told seven years ago to remove lower right premolar and replace this tooth by an implant supported

Good Prognosis is in the eye of the beholder
Case Study Number 430646 External root resorption associated with chronic apical periodontitis altered the shape and position